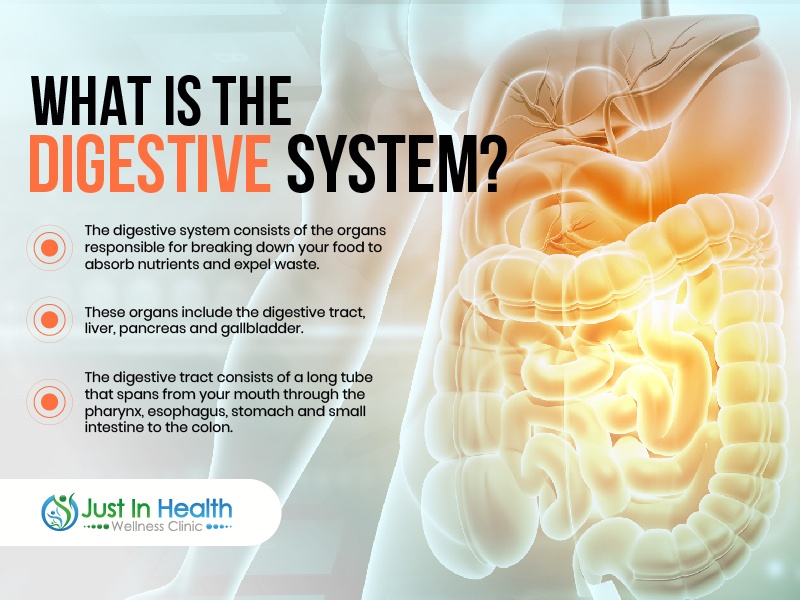
The digestive system is a winding and extensive part of the body. It ranges from the mouth to the rectum. The digestive system assists your body in absorbing vital nutrients and is responsible for getting rid of waste.
Because there are so many types of digestion issues, you might mistakenly dismiss them. Dr. J and Lisa emphasize that it's essential to understand the root cause of digestion issues — as well as emergencies — so you know when to talk to a functional doctor and have yourself tested.

Dr. Justin Marchegiani
In this episode, we cover:
0:00 – Introduction
3:31 – GI MAP Interpretation from a sample patient

![]()
Dr. Justin Marchegiani: Hey guys it’s Dr. Justin Marchegiani here. I am with Lisa Pomeroy. Really excited to have her on today’s podcast. We’re gonna be chatting about different kinds of lab tests. Everything labs really. Our goal today is to show, we’re gonna be really diving into the gut tests, really looking at gut function. One of the big tests we’ll look at is the GI map and how to interpret that and some of the big take-homes as we go through that to you know pull out action items as we address patient concerns. And the next one we’ll go into is the ion panel where we’ll get a really good window into mitochondrial function, neurotransmitter function, overall nutrient absorption, gut function, etc. So, really excited to have Lisa on the show today. Lisa, how you doing?
Lisa Pomeroy: Doing good! How about yourself?
Dr. Justin Marchegiani: Hey,doing wonderful. Really excited to, uh, chat with you, very good.
Lisa Pomeroy: Yeah.
Dr. Justin Marchegiani: Awesome. So, why don’t you let people know a little bit more about yourself me, you’re a clinician as well.
Lisa Pomeroy: I am yeah. I am a traditional naturopath. Um, I’ve done a bunch of differential functional medicine training programs. So, you know like, you I’m a graduate of Dan Kalish’s, uh, Kalish spectatorship. So, I love learning and a lot of the learning was something I had to do to try to get myself healthy. Because when we talk about gut issues, I had major gut issues. I mean, as young as seventh grade, I was having ulcer-like pain and unfortunately, no one I went to, knew about H. pylori, knew about testing for H. pylori, treating H. pylori, so I had to suffer in silence for another 20 years with severe stomach pain before I run the test on myself, found I had H. pylori and got rid of it.
Dr. Justin Marchegiani: Wow! That is crazy. What a story.
Lisa Pomeroy: Yeah, I come home from school and drink cabbage juice. I mean, I was that devoted because it’s the only thing that would help.
Dr. Justin Marchegiani: Yeah, intuitively you knew the vitamin you in there was helping.
Lisa Pomeroy: Exactly!
Dr. Justin Marchegiani: Yeah, so you really had to wait a long time, so that’s crazy because you must have so much appreciation for what we all do today. You have a lot of empathy for your patients. That’s great! It’s important to have that.
Lisa Pomeroy: Yeah, I talk to people and we’ll talk about like a five-year-old child or something and I just, you know, I’m just so grateful because it’s like I’m so glad that they have that the parents know enough to be getting this child help so they don’t have to suffer like I did for another 20-30 years with severe gut pain. You know, we find out that they have a nasty parasite in their gut and we get rid of it and they’re not gonna be nutritionally deficient and have all these gut symptoms for decades.
Dr. Justin Marchegiani: Oh, totally. Yeah. And it’s important, I mean obviously out of the gate, the labs are important to give us a lot of information that’s clinically actionable but you know diet and lifestyle, foundational things, a lot of these, you know, we probably don’t need a lab test per se. I mean, it’s good to have it right? I t’s nice to know, like okay, maybe there’s some gluten sensitivity, maybe there’s some inflammation, maybe there’s some immune activation and we should kind of start some diet changes and there’s some foundational things that you tend to find that just generally help most people out of the gates, you know, maybe sugar or gluten. What things you specifically utilize?
Lisa Pomeroy: Yeah, exactly! I mean, we look at the top pro-inflammatory foods in the diet. Most people say gluten, dairy, white refined sugar and ultra-processed foods. You know, those are gonna be some of your top things, where a lot of people will notice a difference, where you can pull it out, you know, you can do a trial where you, you know, you eat whole unprocessed foods, your whole fruits and veggies, roots and tubers, you know, that sort of things. You cut out the dairy you see how you do, so yes, testing can be helpful with that, but some of it can just be, you know, take it out and see how you feel.
Dr. Justin Marchegiani: See how you feel
Lisa Pomeroy: Exactly!
Dr. Justin Marchegiani: That makes sense. Oh cool. Why don’t we dive into some of the GI map testing out of the gates. I got a sample patient here, we’ll pull it up on screen.
Lisa Pomeroy: Okay.
Dr. Justin Marchegiani: We’ll kind of whip through it and we’ll try to keep it actionable. I mean, unlike a lot of shows, you know, you’re a clinician, I’m a clinician, you interact with patients and doctors throughout the week and so we’re trying to get people, real actionable information here.
Lisa Pomeroy: Yeah, great!
Dr. Justin Marchegiani: Can you see the screen here?
Lisa Pomeroy: I can. Yeah. It’s coming through nice and clear.
Dr. Justin Marchegiani: Okay, cool. So, we’ll just kind of start off, um right off the bat here, page one. So, we’re looking at a lot of bacterial pathogens, some parasite pathogens and viral stuff. I’ll let you, kind of take it away with the first part.
Lisa Pomeroy: Sure. So, basically what I want to see on this first page is nothing. You know, these are things that really don’t belong there. So, I want to see that less than DL which stands for below the detectable limit for all the things down the page. Now, some of these, we don’t necessarily need to interfere with, like that E. coli 0157, uh, that one is something it’s an acute pathogen. It’s actually, uh, like a foodborne pathogen and we’ve been seeing a lot of these pathogenic E. coli lately. They tend to peak in the late summer months, so July, August, September, we see a lot of them, just because they’re on the fresh produce, you know, the leafy greens, served lettuce, your basil, your berries. So, you pick them up and so we’re looking for symptoms. Now, this case, this is a very teeny tiny little level E0. So, that is something they either just picked up a very small amount or is mostly on its way out. And that’s where an E. coli like 0157, you know, is something that’s considered transient, self-limiting, it’ll go away on its own. Now, it may or may not give you symptoms. If you did get symptoms, they probably last for less than a week, probably get some diarrhea, some cramping, fever, nausea, that sort of thing. So, sometimes we’ll see these on the report and we go, okay, well, that explains why you had diarrhea two weeks ago, you know, you got a hold of this bug, but, you know, it may not be something we actually need to do something about.
Dr. Justin Marchegiani: But every now and then, you see the 01h57, I mean, you see, that with spinach a lot, these people will die every year with it. So, if it can be serious to people are, have a compromised immune system or gut function, right?
Lisa Pomeroy: Exactly! And that’s what especially the elderly, the young children, they are the greater risk of more severe types of infections and that’s where a lot of times people, you know, and a lot of times they know that were, you know, the time say they got some diarrhea, they run the test, they’re waiting for the results to come back. Usually, those symptoms are going to peak, before the results came back, so they know I’m having severe things are coming out both ends basically. I’m puking, bloody diarrhea. They should know they need to go to seek emergency medical care. And that’s something where, you know, usually by the time, we’re seeing people. Now, most people don’t get that severe, but if they would, they would have sought medical attention. So, usually, we’re seeing the side more like, oh yeah, I had loose stools for two days, I just my gut was a little off, you know. So, we may not to intervene, although, I always look for there’s deeper bigger issues because, really, you know, the body is meant to protect us from these infections, so if you were susceptible to picking up the E.coli on your spinach or your lettuce, you know, where was the stomach acid, shouldn’t that come in and killed what, you know, you ate and went through your stomach or what about secretory IgA, this is marker later on the test that tells you about gut immunity. You know, secretory IgA. Yep, there it is, yep. So, that one, if that’s low, you know, that’s a problem because that can actually engulf pathogens, so they can’t attach to the bowel wall, can take them so the immune system knows that’s a bad guy, we got to get rid of it. So, if you have a good stomach acid, good bile, those are antimicrobials to kill things, if you have a good secretory IgA, that’s your gut immunity, that’s gonna protect you, it’s our first line of defense. So, again, if I see an E. coli, I may not need to do some protocol to get rid of it, it may just go away on its own. But I’m looking for the deeper issues. You know, if you don’t have good stomach acid, you’re probably gonna pick up E. coli again next summer or whenever you again eat something that has it on it.
Dr. Justin Marchegiani: That totally makes sense. I’ll scroll back here to page one, so we can go in order, uh, and then obviously we have some other food poisoning types of bacteria here Campylobacter, uh, Salmonella, we may see in chicken. Do this change anything for you if someone still has something lingering and some gutted gut issues, I mean, you’re still going to try to address it with some herbals when it’s appropriate.
Lisa Pomeroy: Exactly! Yeah. Some of these and there is, you know, research keeps coming out where we’re thinking something like Campylobacter, you know, we think it’s something that just temporarily stays in the gut and then it’s gone. It’s kind of like a hit and run, where it does its damage and then it leaves the gut repairs. But, in some people, they’ve actually done some duodenal aspirates and find that, you know, they can actually find it still in the gut and the person hasn’t had that recent food poisoning incident. So, there is a little bit of a question with some of these, could they actually stick around a little bit longer and that’s definitely a problem too. So, if they show up on a single report, you know, say Campylobacter, shows up, my initial assumption is yeah, you probably ate some chicken or something lately that had it, but if I’m seeing repeated tests, maybe it’s a chronic colonizer or maybe you keep getting food poisoning, maybe you’re eating at some local fast food chicken place that maybe doesn’t have the best quality chicken or again, you have low stomach acid. It takes very few organisms to infect you if you have low stomach acid, so again, we need to look at, is this a chronic issue for repeatedly seeing it. Is this low stomach acid, low gut immunity, something’s wrong.
Dr. Justin Marchegiani: Exactly. And then same thing here, we have different types of sugar toxins which are, these are toxins actually produced by the E. coli, is that correct?
Lisa Pomeroy: Yeah, E. coli was kind of unique in that there’s, they’re all pathogenic E. coli. You can kind of lump them all together that, but they have different mechanisms of actions, different toxins they produce and so they kind of each got their own special name even though you can all just lump them all together, they’re just food borne pathogenic E. colis.
Dr. Justin Marchegiani: That are gonna produce different toxins that would create inflammation.
Lisa Pomeroy: Uhum, yeah.
Dr. Justin Marchegiani: So, either way, you’re gonna be, you know, trying to clean out the diet and use some kind of herbal to kind of knock it down so to speak.
Lisa Pomeroy: Yep, and I look at food quality, I also, you know, because something like, you know, again, chicken could be a source of Salmonella, Campylobacter. If you’re eating conventional chicken versus organic chicken. They found, you know, when they’ve actually done research studies on this the non-organic ones are more highly contaminated with these bugs than the organic plus they tend to be more antibiotic resistance. So, say, if you do get Campylobacter, Salmonella, chances are it’s going to be a very nasty type that’s not going to respond to treatment, if you did need treatment. Um, and then certain, techniques too like, you know, personally I get organic pastured air chilled chicken because there’s again how is the chicken processed, they can put it in a chlorine bath which is just essentially like a fecal soup, they have all of these chicken carcasses just in this big tub of chlorinated water. And so, if you have one contaminated chicken carcass in this big pool, it can contaminate other ones. Versus air chilled, they’re kind of, you know, just single hanging on their own, so again, they’ve done the research where air chilled is less contaminated with these microbes. So again, whether you’re susceptible or not, I mean, I still don’t wanna, you know, I do my best cleaning my produce, you know, buying good quality food. So, we’re looking at food hygiene, food quality, but you know, you do things the little things that you can do, when purchasing these things to prevent your exposure.
Dr. Justin Marchegiani: Okay, cool. We also skipped, I think C. diff out of the gate so C. diff is a bacterial infection, it can, it’s common in hospitals. High levels of antibiotics can mess up your gut and create an imbalance there, um, obviously toxins A and B together tend to be more synergistic and worse than just one. Do you want to add to that at all? Comments to that?
Lisa Pomeroy: Yeah, so a lot of people see this test and they panic when C. diff comes up because we know that C. diff can be a nasty infection. However, we have to keep in mind what this test is measuring, is the bacteria not the toxins. So, what this tells you is that, there’s C. diff bacteria in the gut that carries the gene that would allow it to produce toxin A and or toxin B. Whether it’s actually doing that at the moment is the question. So, what’s defined as C. diff infection is the bacteria are there actively producing the toxins and the toxins are whether damaging the gut causing the diarrhea, the classic C. diff presentation.
Dr. Justin Marchegiani: What is that?
Lisa Pomeroy: Now, a lot of people are actually colonized with C. diff, where the bacteria is there but maybe you have some good guys that are keeping it in balance preventing it from turning on those genes and producing the toxins and so that’s where it’s important to have the good bacteria there to not wipe them out by antibiotics or other things. So, we can’t differentiate between infection or colonization here, you know, this is just telling us, C. diff bacteria is there and you know, we don’t really want it there. Now, if someone does have symptoms that indicate a possible infection, you know, we certainly could do further testing and actually test those toxins to confirm. But a lot of people, if they say, well, I’m constipated, you know, probably not a C. diff infection, you know it’s, if they don’t present like those classic symptoms, it’s probably more colonization which is far more common but I still don’t want it there because it’s essentially lying in wait, waiting for the opportunity, you get a UTI, you take around antibiotics, now again, you killed the organisms protecting against this, so now, you do turn on the gene, get the toxins, get the C. diff infection.
Dr. Justin Marchegiani: So, we have the bacteria that has potential to make this toxin but it’s not necessarily show that the same toxin, they are b is present. It’s more the potential of it based on the bacteria.
Lisa Pomeroy: Exactly! This tells us about the bacteria and not whether toxins are actually being produced.
Dr. Justin Marchegiani: And this Clostridium, isn’t the same as on page two. This one is a little bit different but this is a kind of more the overall class where this is more of the specific type of Clostridium within that class. Is that correct?
Lisa Pomeroy: Exactly! So, C. difficile is a pathogenic organism that’s part of that large group.
Dr. Justin Marchegiani: That family.
Lisa Pomeroy: Yeah, but Clostridia actually has a lot of beneficial butyrate producers. So, this is just picking up, there’s a very small subgroup of maybe more pathogenic potentially harmful ones within the group.
Dr. Justin Marchegiani: Okay. Very good! Excellent! Anything you want to see down here? I mean we have you mentioned a kind of Salmonella, more connected to chicken and eggs, things like that, uh, cholera more waterborne. Anything else you want to say about Cholera or Yersinia?
Lisa Pomeroy: Yeah, so, Vibrio in the U.S. the most common source is actually seafood. So that’s what I’m checking to see if it’s like, okay Vibrio comes up, which doesn’t all that often but once in a while it will. I just check, you know, did you eat seafood recently and it’s always, oh yeah, I had some shrimp and you know, again, may or may not had those acute symptoms but you know often there’s recent seafood consumption. Now, in other countries, it’s more through the water, through, you know, just dirty water that has fecal contamination, here it’s usually seafood.
Dr. Justin Marchegiani: Okay, very good! And then, um, Yersinia, you said, is that seafood as well? That was just the vibrio?
Lisa Pomeroy: That’s just a vibrio. Yeah.
Dr. Justin Marchegiani: How about Yersinia?
Lisa Pomeroy: Yeah, that one can come through many different sources, um, sometimes it could be, you know, even raw dairy products, could be pork, you know, many different sources for food, uh, but this one actually can be a trigger for Hashimoto’s. So, it doesn’t show up.
Dr. Justin Marchegiani: It can.
Lisa Pomeroy: It can, yeah. So, it doesn’t show up all that often but if it does, I’m looking at the thyroid antibodies and other testing or seeing if there's already a diagnosis of Hashimoto’s.
Dr. Justin Marchegiani: Very good! And then parasite wise, we have Crypto, E. histo, and Giardia, which definitely are the big three, right, um, Crypto primarily found in water, E. histo is going to be nasty little amoebic that people don’t know it’s in the top three to five causes of death in third world countries. It’s a nasty little bugger.
Lisa Pomeroy: It is!
Dr. Justin Marchegiani: And then Giardia, as well, which loves to hide in the gallbladder. I’m gonna let you kind of go into those one by one. Quick question, why do they have these parasites here and then on page four, a separate section for parasites? Why don’t they put them all in one spot?
Lisa Pomeroy: Yeah. My thought is that, you know, within the medical community, certain pathogens now are widely accepted as disease causing. So, like, pretty much, I mean a conventional doctor, a functional medicine doctor, they’re all going to say, you know, Crypto, Giradia, E. histo are bad. You know, we don’t wanna see those. Now, Blastocystis hominis, you know, most functional medicine practitioners will say that, that has a lot of potential to cause harm, linked it with Hashimoto’s and you know, hives and IBS. But from the conventional standpoint, they’re not entirely convinced because some people can have Blasto and not have symptoms. So, the ones on page four, there is research supporting that all of them have pathogenic potential but they’re not as widely accepted as a 100% pathogenic unlike the ones on page one.
Dr. Justin Marchegiani: Makes sense. I know a lot of people like Mayo clinic are starting to say, hey if you have Blasto and have some level of symptoms, well, you probably should address it, you know, most people that we see the problem is. Well, what constitutes a symptom from Blasto for instance we know a lot of gut issues can cause extra-intestinal symptoms like fatigue, brain fog, mood issues, sleep issues. So then, how do you really connect the dots? Obviously, we have diarrhea, constipation, acid reflux, bloating, right? But sometimes you get these extra intestinal ones which are a little weird.
Lisa Pomeroy: Exactly! Like Blasto, people say, oh well I have no gut pain, and then I start asking more about their symptoms like, oh well, I do have chronic hives, and I have joint pain and I have, you know, these other symptoms, it’s like. Well, I can show you research study that’s linked that to Blasto. Yes, it’s not a gut related system symptom, but it’s been linked to blasto.
Dr. Justin Marchegiani: 100% Yeah, very good.
Lisa Pomeroy: Yeah. Yeah. So, going over the page one pathogen, so yeah, Cryptosporidium, Giardia, those are actually both small intestinal infections, whereas the E. histo is a large intestine infection. Um, but Crypto and Giardia, often can be from the water, so we do have to look at drinking water and for Giardia, recreational water can be a big source too. So, again, a lot of these pathogens have their seasons. So Giardia, we can see more prevalent in the summer months because people are going in and swimming in lakes and streams and rivers and swimming pools and you know, or going water rafting or you know doing things recreational water parks and you just get a mouthful of water and chlorine doesn’t consistently kill it unfortunately. So, you still could get it or it could be your well water so I was always look to if we see Giardia, what are you drinking, you know, are you drinking well water, is it filtered, you know, are you, do you swim in lakes and streams, ponds, you have a swimming pool, so we always want to look at that because sometimes if there is, if it is well water and it has Giardia and you can often test your water for these bugs too, you know, we wanna make sure we’re getting rid of that source. Um, but yeah, I mean that could be, these can be nasty again. You can pick them up on the food. All of these have what they call the fecal oral route. So basically, if you know, again, it could be animal poop and stuff that just gets on your leafy greens because your cattle farm is next to your lettuce farm. There’s a little runoff and yeah, it’s hard to wash your produce. I mean, I still recommend soaking fresh produce in water with a little vinegar or hydrogen peroxide in it to try to kill those bugs. But even still, I mean, lettuce has so many little nooks and crannies, it’s hard to get it all killed.
Dr. Justin Marchegiani: Absolutely! And we probably want to make sure every patient that we see, the clinician that we see is recommending a good quality water at least a carbon-based one or ideally even at reverse osmosis just really make sure we filter out all those potential parasitic cysts plus water’s got a whole bunch of nasty things in it, like chlorine, like potential fluoride and pharmaceuticals that you want to filter out as well.
Lisa Pomeroy: Exactly! Clean water is a must whether it’s the bugs or the toxins.
Dr. Justin Marchegiani: Exactly! Any other comments on the viral pathogens here?
Lisa Pomeroy: Yeah again, those you know, again, tend to acute rather than chronic colonizers. Although, again, Norovirus, there is some evidence, it could be a chronic. But you know, these will feel often like a stomach flu. So again, you usually pick it up more your food like poisoning. But, some of these, you could pick up, like Norovirus, say you go to a public restroom, you touch the faucet handle and then you eat your lunch without washing your hands. You know, if you touch something with the virus, you put your hands in your mouth, you could pick up something like Norovirus from touching objects too. But, usually feels like a stomach flu.
Dr. Justin Marchegiani: Okay cool. Well, let’s drive into H. pylori here next, um, and also just a little reference range, um, tidbit for a lot of folks here. If you’re trying to figure out the reference range, you see, I don’t know, let’s say. Let’s go on to see where’s a good example.
Lisa Pomeroy: Well, H. pylori, it’s a big one too.
Dr. Justin Marchegiani: Yeah, but if you look at E. coli, you’re trying to figure out where this fits in the reference range. If the exponent is below the reference range, then you got to move to the left. So, this really is .00860 and then if its above, like this, this is e to the five, right, then you have to move to the right to make it just to make it equal, um, the exponents kind of throw a lot of patients off that I, I find when we go through them all.
Lisa Pomeroy: Yeah. Exactly. Yep. And it’s just, it’s in scientific nomenclature, yeah, it's just otherwise, you have a ton of zeros. Yeah. It just cleans up the report.
Dr. Justin Marchegiani: Exactly!
Lisa Pomeroy: And there’s nice, like these are powers of ten, so you can get like powers at tens chart like e3 is a thousand. So, you can go, oh, that’s e3 is a thousand, take the 2.9 multiply it, that’s 2900 cells.
Dr. Justin Marchegiani: Exactly! Exactly! And then really quick here with the H. pylori. I haven’t seen the last year so a ton of virulence factors come back on my patients. Have you seen that as the lab kind of tone down the sensitivity with that? Have you noticed?
Lisa Pomeroy: It depends. Fortunately, we don’t see them often, which I mean the problem with virulence factors is they’ve been associated in the literature with higher risk of gastric cancer, gastric ulcers, cardiovascular disease. So, if you have H. pylori that has these attached to it, it has more potential to cause harm and disease. Now, I just saw one yesterday, where she has a history of H. pylori and unfortunately, she got it back again and she had it pretty much looked like this one. It had like four or five virulence factors, which is what she was dealing with before too. So, we do still pick them up, you know, again, fortunately, it’s not as often because this is the really nasty type of H. pylori, you don’t want to see.
Dr. Justin Marchegiani: Exactly! And then, regarding the reference range, this is above one. If someone is borderline or a little bit below, would you typically want to treat them or let’s say if they had symptoms, would you still want to treat them?
Lisa Pomeroy: Yeah. So, it becomes more of a clinical decision if it’s below that of a thousand cell threshold. But we have had people have like, this is a 2.9 e3. We’ve had people like a 2.6 e2, which is just 260 cells. They’ve had endoscopies and have been told that their stomach was covered in H. pylori and highly inflamed. So, sometimes, this can be the tip of the iceberg. We have to remember where is this infection located. This is a stomach infection. So, something in the stomach, you know it depends on how much is being shed into the GI tract that day. It’s got to travel 20, 22 feet through the intestinal tract to come out the other end. So sometimes, this is going to be heavily diluted from what we started out with. So, this could, yeah, so this could be a glimpse of what’s there. So that’s where there I, you know, it comes down to the clinical decision, does this fit. If someone comes in and they have gas and bloating and GERD and reflux and stomach pain and I see a borderline level, a moderate positive, I’m probably gonna do a protocol because it fits. Now, if this was a very low level and they had absolutely no symptoms and I looked through the rest of the report, their microbiome looks good, their enzymes look good, their gut immunity looks good, maybe it’s okay. Maybe they have good Lactobacillus and things keeping it in check. But I wanna see signs that it’s not causing any harm so that’s where I look at the symptoms, the history, the rest of the report.
Dr. Justin Marchegiani: That makes sense. And then with these cytotoxic proteins, are these more genetic type of risk factors because of the, because of the genes or are they specifically connected to the H. pylori and if you knock down the H. pylori, will knock down these cytotoxic proteins?
Lisa Pomeroy: Exactly! So, these are genes attached to bacteria. They’re not related to the person. So, as you kill the bacteria, the virulence factors go with the bacteria.
Dr. Justin Marchegiani: Got it! You can clear them as the bacteria gets knocked down. You can, you can knock down the bacteria that has those genes attached to it.
Lisa Pomeroy: Exactly! Like, if you have babA that just allows the H. pylori to stick to the stomach a little bit better. So, we have to, we might bring a little cranberry juice because that has an anti-adhesive property to it. So, we just try to undo that little trick that the H. pylori has which here, the babA allows it to stick so we’re going to do something so it can’t stick.
Dr. Justin Marchegiani: Oh, would that be a good recommendation if you had H. pylori without the babA?
Lisa Pomeroy: You could actually because there is research that shows that cranberry juice seems to kill H. pylori and just prevent it from ticking to the stomach wall. So, with babA, I definitely would include it but I also often include it just with H. pylori.
Dr. Justin Marchegiani: And then, if you address someone like round one and there’s still some H. pylori left or you didn’t move it a ton, are you gonna try a second round with different herbs and just kind of mixed them up? How do you address patients where you don’t quite get the result you want the first round?
Lisa Pomeroy: Yeah, and this is when we’re using herbs, especially the herbs we traditionally use things like mastic gum, DGL, Licorice, they don’t have the major impact on the beneficial flora. So, it’s not like we’re going in there with some really super strong herbs a lot of times that will just knock out everything and so we can often use repeated rounds of some of those herbs safely without disrupting everything else. But I have had people were, especially skin conditions where until we get that H. pylori less than DL, their skin won’t clear up. So, for me, I looked to see now if they’re feeling great if we knocked it down and there’s a little bit again, it’s always a judgement call but I’ve seen people with acne, with eczema, where until it hits a less than DL, they have the symptoms, the second they hit less than DL they’re gone.
Dr. Justin Marchegiani: So, are there any other herbs that you’ll pivot off the mastika or that you use synergistically with it or that you’ll rotate in if first round didn’t work that you’ll pivot on the second or third round with?
Lisa Pomeroy: Uhm. Yeah. So, a lot of times other organisms can actually promote the colonization of H. pylori like yeast is a big one I look for because there’s, yep yeah, and there’s actually research that yeast and H. pylori have what researchers call an intimate relationship. So basically, if there’s yeast and H. pylori together in the mouth or the stomach, the H. pylori can go and hide inside of the yeast and kind of seek refuge inside of it and then later come out when the coast is clear. So, if I see a bunch of yeast on the next page, I may need to bring in some antifungals at the same time trying kill H. pylori or it’s just gonna hide out and just come out later. So, that can be something we miss, you know, H. pylori can produce biofilms and hide inside a yeast. Some bacteria can produce hydrogen and that hydrogen also can fuel the growth of H. pylori. So, that’s where sometimes I do look at. Okay, let’s bring in some Berberine, some Oregano, some Neem, some Pau D’Arco silver, something that’s gonna also address the bacteria or the yeast or some biofilm disruptors like NAC, and acetyl cysteine, can break down H. pylori biofilms. So, I’m thinking about all of those things because those could be what we’re running into a wall.
Dr. Justin Marchegiani: Makes a lot of sense. Very good. Any of the comments on the H. pylori and then also like what are the big virulence factors to look out for, like a top three?
Lisa Pomeroy: Yeah, I mean, some of the nastier ones we’re thinking more like gastric ulcers, gastric cancers, cagA is one of those big nasty ones. Um, dupA, the dup is duodenal, so that one’s a little more duodenal ulcer. VacA, that again, is another one, where ulcers, cancer. So, I’d say, the three worst one, the cagA, dupA, the vacA. I mean, yes, babA is not a good thing but it’s more allowing it to stick to the stomach a little bit more, it’s gonna be a little bit invasive, a little more inflammatory. But, you know, those other three are just especially nasty.
Dr. Justin Marchegiani: Got it. The cag, the dup, and the vac?
Lisa Pomeroy: yeah
Dr. Justin Marchegiani: Okay. Very cool. And now we go into the normal bacteria. These are commensal flora, normal flora in the gut but we can kind of gain a little bit of insight what’s happening in the gut based on these imbalances. I mean, out of the gates we have, you know, just out of the gates, we have Lactobacillus, which is a beneficial flora that’s low so we’re certain starting to see low levels of beneficial bacteria. Anything you want to say kind of from this section down?
Lisa Pomeroy: Yeah. And again, we can tie this with other sections too like Lactobacillus actually lives in the stomach and it’s very antagonistic towards H. pylori. So, if I’m looking at this and going well, we have a nasty H. pylori and infection, we have low levels Lactobacillus, I’m gonna get, get a lactobacillus probiotic in here, to try to help not only get more Lactobacillus in the system because it’s clearly lacking but it’s gonna help push out some of that H. pylori from the stomach. Now, in general, I look at, you know, do we have highs, do we have lows, because even though these are good guys, too much of a good thing is a bad thing. So, I still don;t wanna see highs or lows. Now, lot of times, when things are low, it’s often something killed them. So, I look for a history, did you take antibiotics recently or things like artificial sweeteners, like you know, splenda, sucralose, it’s a chlorinated sugar, chlorine kills bugs including the good bugs, so we need to be looking at agian the diet. Are you doing something that’s killing these, do you eat GMO foods, food sprayed with glyphosate? Glyphosate is patented as an antibiotic, again it’s gonna kill your good bugs. So, are you doing something that’s killing them or are you starving them, you gotta feed your bugs, they like fiber, so if you’re restricting fiber in your diet, if you’re not eating lots of whole fruits and vegetables and beans and nuts and seeds and you know maybe some gluten-free grains. I mean all of these things have the fibers that these guys love.
Dr. Justin Marchegiani: 100% and so a lot of fibers, a lot of fruits, a lot of vegetables. If someone were to go carnivore, would you see a lot of these commensal flora drop typically?
Lisa Pomeroy: You do, unfortunately. Yeah. Unfortunately, we have seen some reports for people who are doing carnivore and especially if there’s low stomach acid, especially if there’s H. pylori, you’ll see, a lot of the ones, the opportunistic ones on the following page go really sky high and you’ll see lots of low levels here because these guys like their fiber. Now we don’t test some of the bile loving bugs here but you know if you were testing those, we would expect to see some of the protein degrading, you know bile loving ones, those are the ones that are gonna go up but they’re also ones that produce things like hydrogen sulfide which can be very pro-inflammatory in excess. So, while it may relieve some symptoms, I’d rather look at why can’t you digest your foods and vegetables and carbs and that kind of stuff. You know, there’s probably an infection like H. pylori or some dysbiosis instead of restricting your diet so severely and starving your good bugs, let’s get rid of these bigger issues, get you digesting better so you can have those foods again.
Dr. Justin Marchegiani: Very good. And so, out of the gates there, any specific changes that you’re gonna see, you’re gonna make outside of those recommended diet or lifestyles? Things for like Faecalibacterium prausnitzii, Akkermansia, any specific changes there?
Lisa Pomeroy: Uhum, yeah. So, Faecalibacterium prausnitzii is the major butyrate producer, so butyrates are very anti-inflammatory in your gut but it also has an effect in the brain. Butyrate produced in your gut will cross your blood brain barrier and have an anti-inflammatory effect in your brain, stimulates BDNF – Brain derived neurotropic factor, can help with anxiety. So again, we’re not just looking a gut impact here, we may see this is low with skin conditions and anxiety and all these other issues. But this loves fiber, loves resistant starch, so I might suggest, you know, let’s eats some, you know, rice that’s been cooked and cooled or some potatoes or roots and tubers that have been cooked and cooled because if you cook these foods and then you cool them it creates resistant starch. So, like something, like potato salad would, you know, Faecalibacterium prausnitzii would really happy with some potato salad. But also your fibers, you know, fruits and veggies, roots and tubers, all of that stuff but it wants fiber.
Dr. Justin Marchegiani: Very good. And what if some of those foods cause people to get more bloated or gassy like let’s say they have issues with nuts or have issues with legumes or lentils, would you suggest they continue to eat that even if they feel bad or listen to their body in that?
Lisa Pomeroy: Yeah. We always want to listen to the body, you know, some foods are just harder to digest than others so some people especially if your gut is very damaged and inflamed, maybe you can’t handle the beans, legumes, lentils right off the bat. So, we find different foods, you know, other fiber-rich foods that don’t cause that discomfort and sometimes it’s about portions too, so something like an apple. Maybe you can’t have a whole apple because it has a lot of fermentable carbs but you can have two apple slices or you can’t have a whole plate of asparagus but you can have two spears of asparagus and a stir fry. So, we’ll always look at those things but I also look at enzymes. You know, if you don’t have enzymes to break down these foods, you’re probably gonna feel too good with them. So, I’m always looking at elastase, one again later in the report if that’s low. I’m bringing in a pancreatic enzyme supplement because that not only helps with your gas and bloating and you know all those digestive symptoms but also helps of the dysbiosis because if you’re not digesting your food, your bugs will, so you’re giving them all you can eat buffet if you don’t digest your food. So, enzymes are really key and they’ve actually done some really cool studies finding that, that low elastase one is actually a more influential on your microbiome than your diet and all these other factors. You know, having poor digestion will highly influence what’s growing and not growing.
Dr. Justin Marchegiani: Very cool. Anything else you want to say about, um, the different families of bacteria so the conventional thinking is Bacteroides is very helpful very important to have in your tummy in good amounts, uh, Firmicutes the high levels of this one tends to so that you know the B for Bacteroides, B for beautiful, very beneficial. Firmicutes, one of these ones where high levels increase calorie extraction which potentially some correlation with weight gain in the literature. Any comments on these?
Lisa Pomeroy: Yeah, so again, it’s all about balance. So Firmicutes is actually where a lot of those butyrate producers are. They’re in this category. So, both, you know, we can’t say that either one is good, one is bad but good guys and bad guys in both categories so it’s just all about having that balance there. And yes Firmicutes, they can, you know, make you retain more calories from your food so you could gain weight, if they’re abundant but I’m looking at if your Firmicutes is getting too high it’s probably you’re eating too many carbohydrates or you’re not digesting them. So again, if I see this high and your enzymes are low, I’m getting those enzymes in there and we’ll often see this balance out.
Dr. Justin Marchegiani: Yeah. And then, you may want to address either fermentable, FODMAPs or even go lower carb as well?
Lisa Pomeroy: Yeah, depending on it again, I look at symptoms, I mean I don’t want to starve the colonic bacteria, so I’m just, you know, a lot of times just finding which fibers are triggering symptoms, can we get some enzymes in there. There’re actually enzymes now that are specific for digesting high FODMAP foods and so I’ll bring in something like that where you know they’ll say, we’ll I love onions, but you know I just get such terrible gut pain afterwards. You take this enzyme, you can eat onions. So, your microbiome, loves onions, you know. Yes, they are highly fermentable they can cause more symptoms but if you get the proper enzymes in there, a lot times you’re fine and your gut microbiome will thrive on those foods. So, I’m very careful about what I take out, because you know, I don’t want to trigger symptoms but I also don’t want to starve bacteria.
Dr. Justin Marchegiani: Um, very good. And then what about increasing Bacteroidetes, is anything specific to help with that?
Lisa Pomeroy: Yeah, so maybe again, it’s something you know, if they’re low we think about, you know, fiber again the whole like more plant-focused foods but something too we know about Bacteroidetes, they don’t like excessive fermentation, so that’s where again, I look and connect the dots here. H. pylori showed up, H. pylori in most people causes low stomach acid. If your acids low, you’re probably excessively fermenting your food. Bacteroidetes don’t like the pH shift that occurs as a result of that, so they’re just not going to do well. You know a lot of these bugs what’s growing is going to be determined by pH and oxygen levels. So, chances are, you know, if you get some plenty of fiber in the diet get rid of that H. pylori that’s suppressing the acid causing excessive fermentation, these again could just balance out.
Dr. Justin Marchegiani: Very good. Excellent. And anything else? Let’s hit the dysbiotic bacteria section. So, these are quite frequently going to be found in general dysbiosis or SIBO right? Um, Bacillus is kind of this beneficial spore like probiotic that you get in megaspore or thrive or lot of these newer probiotics that are out. Why don’t you take it from there so with this one there’s a certain threshold that you like to see it stay below but if it’s a little bit high, is that okay?
Lisa Pomeroy: Yeah. So, bacillus actually, a healthy gut should have some Bacillus in it so this is one we actually see a number next to that Bacillus species on every single report. So, an e4 e5 is actually pretty typical. With this one, I’m actually more concerned if I see a less than DL. To me, that’s more of a deficiency of this. So, you know, if it’s low, I mean, again we think about the diet and all those things we can supplement since we do have them available in probiotic form. Now, if it’s high there’s been a link between poor digestion and excessive levels. So, if it’s going high, I tend to think, okay what’s going on with stomach acid with enzymes with all of those things. So, that’s what I’m usually supporting if it’s getting high.
Dr. Justin Marchegiani: Very good. Excellent. Probiotic, enzymes if it’s getting high. Anything else with restriction of carbohydrate or FODMAPs at all?

Lisa Pomeroy: With that one, I don’t usually do too so much. It’s more just uh focusing on if something’s causing low stomach acid like H. pylori. We need to deal with that bigger issue but it’s often more just poor digestion, digestive dysfunction.
Dr. Justin Marchegiani: Very cool! Anything you want to say about the general dysbiotic bacteria below? We can start with the despotic section. I mean, is there any rhyme or reason of why one may proliferate in someone’s gut over another or is it just kind of the dumb luck of you know, too much sugar, too much carbs, antibiotic exposure, not cough beneficial flora to compete? How does like, why would one proliferate over another?
Lisa Pomeroy: Yeah, so there’s definitely certain conditions that will promote some over others. Like we see, Klebsiella there in that bottom section. It not only causes inflammation but it loves inflammation. If your gut becomes inflamed, it’s going to bloom. So, with this one if your gut is inflamed because you have a, you know, crappy diet because eating a bunch of food additives and proinflammatory foods. You’re lacking those good butyrate producers. You know, all of these things have changed in your gut to make it inflamed that’s gonna make your Klebsiella very happy and it’s gonna become overly abundant like this or things like, you know, certain things have been tied in the research with low stomach acid. So Streptococcus, you know, one of the top things, you’re going to see with low stomach acid again this individual is dealing with H. pylori. So, we’re probably going to see some high Streptococcus, which we do. Besides Streptococcus, Staphylococcus tends to show up with low stomach acid. Again, right above that there it is and Enterococcus. Now, Enterococcus here was more a moderate overgrowth but still it is showing up a little bit which it’s fitting with this pattern. The more things that you have showing up that fit that pattern the stronger it is. So, I’d say, the enterococcus, the Staph, the Strep, Klebsiella will see more with low stomach acid and even Pseudomonas. Pseudomonas thrives when there’s a lot of undigested protein around. So that’s another one where, this page to me looks like a classic consequence of having low stomach acid. So again, we have to think upstream what’s causing them, that correct that but we also may bring in some antimicrobial herbs because this has gotten to such a state where we may not be able to just get rid of these by dealing with those bigger upstream issues like H. pylori and low enzymes at this point.
Dr. Justin Marchegiani: So, the Enterococcus, Staph, Strep, and Klebsiella, when you see them elevated, there’s going to be more of a connection with low stomach acid and probably low enzymes too because those are connected as well right?
Lisa Pomeroy: Exactly! We often call this the digestive dysfunction pattern.
Dr. Justin Marchegiani: Okay. How do artificial sweeteners impact this or even things like pesticides will they have a kind of negative impact like an antibiotic. How does that work?
Lisa Pomeroy: Yeah, they can. That’s what they find a lot of the artificial sweeteners they find that they tend to kill things like Lactobacillus and Bifidobacterium, and yet they promote a lot of times it’s this one other phylum which is called Proteobacteria, so Klebsiella is a member of Proteobacteria. Pseudomonas is a member of Proteobacteria. But they’re really virulent, more proinflammatory organisms that will tend to bloom again with more inflamed conditions higher oxygen and they also tend to go up when we have food additives and chemicals and pesticides and all of that. So, you see a lot of the research, it’s kind of like the, the bad dysbiosis pattern you’ll see is these high Proteobacteria, like again, high Klebsiella, high Pseudomonas, with low butyrate producers like for Firmicutes, low Clostridia, low Faecalibacterium prausnitzii. So too many proinflammatory bugs not enough anti-inflammatory bugs.
Dr. Justin Marchegiani: Got it. And so lower butyrate, uh, not enough anti-inflammatory bugs and that’s more with what Provatella, Proteus, Fusobacterium, was the big ones there?
Lisa Pomeroy: Those are gonna be your more proinflammatory ones again. Yeah. Anything in your potential odder will trigger susception.
Dr. Justin Marchegiani: with low butyrate
Lisa Pomeroy: With low butyrate, yeah. Because that’s going to change the environment that will promote their growth.
Dr. Justin Marchegiani: And so, when you are working on producing butyrate, can things just like butter which is butyric acid, can that have an influence? Are you trying to also add in potential resistant starch or probiotic fibers or adding just actual Butyrate in there? What are, what are your thoughts on each one of those and what do you do to try to impact butyrate?
Lisa Pomeroy: Sure, yeah. I mean, butter or ghee it does have some butyric acid or butyrate. It’s just, it’s so small, it’d be hard to get therapeutic amounts plus a lot of people are dairy sensitive especially when their gut is damaged and leaky.
Dr. Justin Marchegiani: Can be for sure
Lisa Pomeroy: Yeah. So, if I’m going to supplement or try to get more butyrate in, I look at, I mean, we could use a tributyrin supplement, you know that can be really great like if I see, if all the butyrate producers are low and their calprotectin is high which is telling me their gut is inflamed and they have a lot of GI discomfort and they also have a lot of food sensitivities. Getting that butyrate in there directly can often calm things down or diarrhea. Butyrate can be terrific for diarrhea. We’ve seen chronic diarrhea that’s been going on for years or decades. Stop within a week of giving some tributyrin. So, sometimes I do give butyrate directly or IBD I’ll often use some butyrate directly because the gut is so inflamed that can be really helpful. But a lot of times, you know, people don’t necessarily want another supplement. You know if I’m not seeing those major signs where I definitely want to add it in, I may just be let’s feed the butyrate producers. Yes, we can give the end product but you’re still not feeding them, you know, I always think of like the butyrate is more like giving you healthy soil that’s going to promote their growth but you still got to feed them. They’re not gonna grow if you don’t feed them. So, you got to get the fiber in there, so I look at, you know, you can feed them with the fiber, you could get the butyrate in there and maybe you want to do both. They find that actually giving the butyrate and the fiber which is promoting the environment and giving the fertilizer to feed them, you get an even stronger impact. So many different options what we may do, any combination of those.
Dr. Justin Marchegiani: So, if it’s only those bacteria are in the lower sides. If they’re higher, would you also still want to do that?
Lisa Pomeroy: Depends what we’re seeing, I mean, again, if the gut is highly inflamed, I may bring it in or there’s terrible diarrhea, I may do it more for symptomatic relief. But, you know, if those bacteria are in good shape, you know, we don’t necessarily need to do that to encourage them to grow by shaping the environment but there’s still other reasons, we might use butyrate.
Dr. Justin Marchegiani: Is it more of a concern when they’re higher or lower?
Lisa Pomeroy: It’s low that it’s more there’s usually a deficit of the short chain fatty acid butyrate if they’re low because if there’s low population, they’re not making enough butyrate
Dr. Justin Marchegiani: That’s less than DL you’re looking at, right less than DL
Lisa Pomeroy: Yes, these aren’t the butyrate, those are on the previous page, um.
Dr. Justin Marchegiani: You’re talking about the commensal stuff here.
Lisa Pomeroy: Yep. Yeah. So, the three markers that represent them are the Firmicutes phyla, at the very bottom. Yup, the Clostridium class and then Faecalibacterium prausnitzii.
Dr. Justin Marchegiani: Okay, got it. These are the big three, Clostridium, Faecalibacterium and Firmicutes, these are the big butyrate producers.
Lisa Pomeroy: So, there’s low, if they’re low you just could try feeding them or if the guts really inflamed again, they don’t like an inflamed environment so you may bring the butyrate in to try to take down some of the inflammation and then give them the fiber and now they’re really gonna grow.
Dr. Justin Marchegiani: Got it. Okay. Very cool. Anything else you want to say about the like Citrobacter or these despotic bacteria individually, I mean, a lot of these are gonna be commonly found in SIBO right, but because it’s a stool test and all of it, it’s moving through the intestines, we wouldn’t necessarily say this SIBO unless we had like a breath test but we could say that’s a kind of a generalized dysbiosis.
Lisa Pomeroy: Yeah. And some of these bacteria we look at like Klebsiella, Pseudomonas, they just live in the small intestine that’s just their area that they hang out but it’s not necessarily SIBO, you know, yes, they’re in the small intestine but SIBO is when there’s too many overall bacteria in the small intestine, sometimes you just have a dysbiosis. You know, it may just there’s not, overall, it’s just Klebsiella and Pseudomnas are too high.
Dr. Justin Marchegiani: And so, you’re gonna utilize like a breath test, a lactulose, where you’re looking at hydrogen and methane gases and see if they’re really elevated to really know that.
Lisa Pomeroy: Yeah. If you wanted to see more of that SIBO picture, is there too many bacteria in the small intestine because maybe you had food poisoning incident before and your migrating motor complex that kind of that street sweeper isn’t working well to push the bacteria out. But if I’m looking at these, yes, these are in the small intestine, they’re overgrowing you know, maybe there’s other things overgrowing in the small intestine with them but you know to me it’s something, I’m looking at, you know, low stomach acid, low enzymes, is a huge factor with bacteria in the small intestine. So many cases, we can work on digestion, H. pylori, get some antimicrobials in there and often takes care of those whether even though, they’re in the small intestine versus a colon.
Dr. Justin Marchegiani: Cool. Anything else you wanna say about these individual dysbiotic critters?
Lisa Pomeroy: Yeah. Well, Klebsiella, since this one shows up, these are, you know, besides being very proinflammatory, they are putting, you know, putting you at increased risk of perhaps developing autoimmune condition. So, like Klebsiella is something that’s been linked with rheumatoid arthritis, ankylosing spondylitis, IBD. So, if you had that perfect storm, if you have the bacteria which is your trigger, you have a leaky gut and you have the genetics that make you predisposed to getting say rheumatoid arthritis. It could lead to that down growth. So that’s we’re seeing signs, you know, maybe you don’t have rheumatoid arthritis now, but 10 years, 20 years, 30 years from now, if you don’t do anything about Klebsiella, it could turn into that. So that’s where again we look from a functional medicine perspective, you know, we wanna try to head off a lot of these symptoms too and that’s where we can get a glimpse into that now, with the stool testing to try to get rid of this. Now, so it doesn’t become a future problem.
Dr. Justin Marchegiani: Very cool. Anything else you wanna say on these down below the Proteus or the Fusobacterium?
Lisa Pomeroy: Uhm. Yeah. Now, some of these actually live in the mouth, so Klebsiella lives in the mouth, Provatella lives in the mouth, Fusobacterium lives in the mouth. So, we can’t forget other microbiomes too. So, they’re part of the oral microbiome. And there’s actually a lot of overlap. I think it’s like 45% of the microbes are similar between the two. So, we always have to look at oral health, dental health, if someone has issues in their mouth maybe they need to get their teeth cleaned, get an infection dealt with. Because if you’re swallowing these bacteria every day in your saliva. Now, if you have low stomach acid, you don’t kill them very well as they pass through the stomach so you could get too many in your intestinal tract because there’s low stomach acid but you could also too many in your intestinal tract because there’s too many in your mouth. So, we have to be always looking at the health of the mouth too and what’s coming above the GI tract.
Dr. Justin Marchegiani: I’m a big fan of flexing either with colloidal silver or hydrogen peroxide and if you’re sensitive you can always dilute at 3%, that’s very helpful at knocking down some of those bugs, do you agree?
Lisa Pomeroy: Exactly. Yeah. Exactly. A lot of people like water picks and they’ll do different things and mix and sometimes they’ll alternate too and yep and even the nasal, I mean you have to figure, you know, what’s you know, is being swallowed there from the nasal passages.
Dr. Justin Marchegiani: Post nasal drip stuff
Lisa Pomeroy: Yep, we’ll squirt some silver or something up to the nose too to try to kill something that’s in there, that’s being swallowed and getting down in the gut.
Dr. Justin Marchegiani: Very good. Let’s dive into yeast. I typically don’t see a lot of yeast come back on these labs. When I do it’s usually beneath the reference range sometimes it’s positive but a lot of times I tell patients, if I see it here and it’s not DL then it’s probably a concern. I mean on the organic acid testing which we can talk about at a later point we’ll see things like D-arabinitol or D-arabinose, which is a really good yeast, uh, marker which does, I do find that tends to come up a little bit more frequently than, uh, this test. What’s your take here?
Lisa Pomeroy: Yeah. So, yeast again, we have to keep in mind, it can grow lots of places. You know, it can grow in the mouth, in the stomach, in the small intestine, in the large intestine
Dr. Justin Marchegiani: Skin, Fingernails
Lisa Pomeroy: The skin, yeah. So, I mean of course, anything outside of the GI tract is not gonna show up in the stool. If you have a toenail and fun-fungal infection a scalp fungal infection. It’s not gonna come out in your poop unless it’s also in your gut. So, we always have to keep in mind people say oh I have a yeast problem at my toenail, why didn’t it show up. It’s like probably localized to your toenail. Now, of course, again, we have the dilution factor. If you have thrush, if it’s more in your mouth and not so much in your colon, we may not see a hug amount in the stool or even in the stomach because it’s gonna be diluted out as it travels, so this is really good at looking at like especially the lower bowel because it’s right there ready to exit. The higher up in the GI tract you get, the more dilution is going to play a role into it. Where sometimes maybe you will see it more in organic acids in a urine test than in the stool. If it is a little more upper GI. although, I mean we do pick up DNA that’s coming down from the mouth, the stomach as H. pylori shows up small intestine. But this is something where if it’s detected at all to me that’s a problem because yeast overgrowth tends to cause a lot of symptoms especially hits the gut and the brain. So, a lot of people will say yeah, I have the gas the bloating, you know, the constipation, the diarrhea but it’s also the brain fog, the memory loss, I can’t remember where I put my keys, it’s no cognac, I just, my brain doesn’t work like it used to.
Dr. Justin Marchegiani: The acetaldehyde produced from Candida right?
Lisa Pomeroy: Exactly. Candida produces so many toxins, a lot of those affect the brain or they have the, the sugar cravings so it’s like, I want to get healthy and I want to stop eating all these carbs and candy bars and everything but I just can’t, you know, It’s the Candida calling out for. So, you gotta knock out the Candida.
Dr. Justin Marchegiani: On the extreme side, you could have auto brewery system, um, syndrome, when you’re actually creating your own fermentation with it. The story of this is true, a gentleman got pulled over and he was tested being drunk on the breathalyzer but it was actually yeast in his gut that like made their own little brewery in there and created alcohol from that metabolism that got him drunk and a lot of cognitive people that feel drunk, feel brain fog, it could be from that yeast and all that fermentation happening
Lisa Pomeroy: Yeah, and other organisms can do that too, Klebsiella, another one that could do that too.
Dr. Justin Marchegiani: Ah, interesting. Good, very cool. And then, does it matter, I mean obviously Candida tends to be the bigger yeast most people know about that and you have some subspecies here. Any difference is it, does it matter, are you treating them the same way? Do they differentiate in symptoms at all?
Lisa Pomeroy: Yeah. It’s hard to say in symptoms I mean a lot of the yeast behave the same, a lot of times we’re doing similar protocols anti-fungal, you know, fatty acids like caprylic acid, undecylenic acid, herbs like Pau D’Arco, berberine, oregano, so we’re typically addressing them the same. Now, these are all can be normal inhabitants of the gut like Candida, it’s, you should have Candida in your gut. You know, it has a purpose, the whole thing is it’s all about balance. You get too much of it creates all these toxins and excess you can get symptoms. So same thing with these and some of them are actually in your environment like Rhodotorula is something that we sometimes see a little bit of that showing up and certain areas of the country seem to have it more just in the environment. It’s kind like a pink colored fungi. So, I tell people like do you have like a pink colored ring around your toilet or your tub something like that in your bathroom, it could be Rhodotorula.
Dr. Justin Marchegiani: Interesting. Anything else in this?
Lisa Pomeroy: That’s the main thing with the yeast there. Yeah.
Dr. Justin Marchegiani: How about the viruses?
Lisa Pomeroy: Yeah. So, the main reason, the viruses are on the panel is when these viruses are reactivated in the colon, they’ve been linked with IBD. So, we’re looking for that association there with you know colonic viral reactivation. Now of course we know that these viruses can live in many organs and tissues like Epstein-barr virus and the thyroid gland. So, it doesn’t mean if these don’t show up that you don’t have the virus somewhere else in your thyroid, liver but this is looking more of the IBD colonic link.
Dr. Justin Marchegiani: Very cool and we have different parasites as well, we kind of already chatted about Blasto earlier, but can you give us kind of the reader’s digest from on the critters here, on the bugs.
Lisa Pomeroy: Yeah, so again, all of these can cause symptoms in some cases very severe now these the ones I’d say tend to cause the worst symptoms, would be the Blastocystis hominis and Dientamoeba fragilis. Especially in kids, we can see, you know, kids with just terrible tummy aches and pain and issues maybe failure to thrive they’re just a little underweight for their age and you know, just a lot of behavioral issues. We see Dientamoeba fragilis come out a lot. Both the Blasto and D. fragilis have been linked with IBS and studies. So, we do often see some quite significant symptoms with them. Uh, now some of the oddball things, extra intestinal you may see, you know, with like joint pain, I think, Blasto and Endolimax nana is another one. I’ve had a lot of people where it’s like I think I have Lyme disease and so we’ve run a lot of good because Lyme disease, you need a good test because it’s hard to find. But if you do a good Lyme disease test, you know, when it comes up negative, you know, we’ve had people do that and it’s like, we’ll it’s negative what do I have, I mean, this joint pain is awful and it’s Endolimax nana, so it has affinity for collagen related tissues, so you can see some pretty nasty joint muscle tendon, ligament issues with that one.
Dr. Justin Marchegiani: This is more collagen based huh?
Lisa Pomeroy: That’s the Endolimax nana.
Dr. Justin Marchegiani: Oh yeah.
Lisa Pomeroy: Yeah, yeah so that’s what I look for with that one well I’ll, you know, if I see it show up and they’ll say well I have no gut symptoms. It’s like, well when you work out at the gym, do you see an injury prone where it’s like oh I was lifting weights and now I twisted my shoulder and oh, now it’s trying to run and now my ankle hurts and you know or they just go I’m you know 29 and I work out, I go for a run and I’m so sore and stiff in the morning. I don’t think I should feel like this for 29 years old.
Dr. Justin Marchegiani: Exactly.
Lisa Pomeroy: Yep.
Dr. Justin Marchegiani: Very cool. Anything else on these Pentatrichomonas at all?
Lisa Pomeroy: Yeah, I mean again, some of these just vague, just general gut related symptoms. You know, any of these really could cause gas bloating, abdominal pain, discomfort, constipation or diarrhea. So you know, just general like IBS type symptoms.
Dr. Justin Marchegiani: Very cool. Anything about the worms? I don’t see the worms come back as much. I really don’t. Do you?
Lisa Pomeroy: Well, we don’t see a lot of worms, you know, fortunately because they are a little trickier, you know, we often do recommend deworming medications because it is very difficult to kill them with natural means. But yeah, worms can be quite nasty, um, you know, some of these are, you know, small intestine too, and things like the you know, Ascaris is a roundworm, you know, it doesn’t, you know, some of these worms like the, the hookworms and things, they actually attach to the bowel wall, so they kind of stay in place, I mean, they could, you know, suck your blood and stuff, you know, get the nutrients from the blood. But Ascaris is kind of free-floating there and the problems is because it’s free-floating, it’s not attached, it sometimes gets into places where we really don’t want it and so they found it migrating into things like your gallbladder and you know, your lungs and other places so that one, I mean the big issue with these worms are they can create blockages in some cases with those big worms, you know, sometimes, there can be blood loss, nutritional deficiencies too because if they’re you know sucking your blood and damaging your gut, you could have impaired nutritional absorption. Now, in the U.S., we typically, don’t see these massive infections where there’s like a big ball of worms but you could have a couple worms and they could be causing a lot of issues. Yeah.
Dr. Justin Marchegiani: Interesting. Very good. And then anything else with the, I think, the Trichuris, that’s the whipworm, right? Um, Nicator, is that a hook I think, not sure hook or whip but either way. Different, different, other different worms there, which we’re gonna treat either with, you know, typical medication like Mebendazole, Albendazole, Vermox, or higher dose wormwood or Artemisinin, also tends to be very helpful with some of these too.
Lisa Pomeroy: Yeah. And again, some of these, they all have different ways you can get infected, like some of them it could be walking barefoot on a sandy beach, you know, others it could be. Yeah. some of those worms
Dr. Justin Marchegiani: Trichuris
Lisa Pomeroy: Yeah. And in others you could be, you know, you’re exposed to it through like there’s pork tapeworms and you know beef tapeworms and stuff so again it’s looking at food quality and making sure that it’s cooked thoroughly. You don’t want to go to a restaurant and get the rare hamburger or be eating, you know, a rare
Dr. Justin Marchegiani: Make sure, its good restaurant, make sure the quality is good.
Lisa Pomeroy: Exactly.
Dr. Justin Marchegiani: Make sure it’s like Wagyu from like a five-star restaurant at least. Yeah, for sure.
Lisa Pomeroy: Yeah.
Dr. Justin Marchegiani: Cool. And then down below, we have a couple of markers here out of the gates. The steatocrit right, which is the marker for maldigested fat, so if we see a lot of fat in the stool we’re thinking of potentially either gallbladder flow issues, maybe stones that are affecting the flow maybe we don’t have enough acids because acid is really important for the gallbladder to trigger and contract make CCK, elastase and another marker for the pancreas and enzyme production and again if you have low enzymes, um, HCl or acids is an important stimulator for making and activating enzymes. Any comments on those?
Lisa Pomeroy: Yeah. So exactly. Yeah. so steatocrit has to do with fat malabsorption. Now ideally, I’d like to see a less than DL here. So, I really don’t want to see malabsorbed fat showing up in the stool. Like this one. Isn’t terrible at six so six percent of the stool was some undigested fat but it’s still it’s not ideal, I’m looking for signs why might that be, is there a bile issue, is there a lipase issue. Those are the major things that are digesting your fat, your bile from them you know, produced by the liver, secreted by the gallbladder or lipase is a pancreatic enzyme so for me then you know, if I see this, I look at the elastase one to go, okey what’s the lipase looking like. Elastase, one healthy control usually above 500. So, this individual, I’d say okay, Lipase is probably a little low because were only 388, so chances are if we get a good pancreatic enzyme in here with a nice amount of lipase, will clear up this fat malabsorption too.
Dr. Justin Marchegiani: Very cool. And then any feedback on the Beta glucuronidase, well that’s a, I mean, we’ll just like talk about it out of the, out of the bat. This one has a major effect from dysbiotic bacteria producing it right and so but it also can affect hormone metabolism so you have these bad bugs maybe it’s Klebsiella or gram-negative bacteria like Proteus or Citrobacter. It’s gonna make this enzyme that is going to take conjugated estrogen and it’s gonna deconjugate it and allow the estrogen to go back into the circulation. Comments there?
Lisa Pomeroy: Yeah. Yeah. Exactly. We look at sources. Now, bacteria is the number one thing I look for. Do we have those species over growing that produce it so then I go flip back to page two and three and go, do we have E. coli, do we have high Bacteroidetes or Bacteroides fragilis, uh, do we have
Dr. Justin Marchegiani: So you may look here, so you may look at Bacteroides, you may look at E. coli or what else? Anything else?
Lisa Pomeroy: Uh, the Bacteroides fragilis, Bacteroides fragilis at the top there. Um, Clostridium class and Firmicutes phylum some species, I mean those are large groups but there’s some in there, if those are high it may also be coming from there.
Dr. Justin Marchegiani: Now, this person doesn’t have a lot of those either and they still have it.
Lisa Pomeroy: They don’t, yeah.
Dr. Justin Marchegiani: Again, it’s a sample but
Lisa Pomeroy: Yep. Now the next page do they have Staphylococcus. Uh, they do and really high, yeah, we have Staphylococcus species. Staphylococcus can also produce it. So, this person, I’d be going, okay maybe the Staphylococcus is the where it’s coming from so if we get the staff down, we could bring this down. Yeah, the problem is especially we look at you know say this is a you know a menstruating female. You know, she’s producing a lot of estrogen and she can’t get rid of that estrogen so they say beta glucuronidase kind of comes around like a pair of scissors so say you know your toxin your estrogen goes to the liver goes through glucuronidation which is a detox pathway and the body kind of packages it up nice and neat for elimination so it puts the estrogen in a box puts the lid on the box ties and nice little bow around the box. Well, your beta glucuronidase comes around like a pair of scissors snips of ribbon, lifts the lid, let’s the estrogen out so now estrogen gets to get reabsorbed recirculate and now you get estrogen dominance so now you have PMS and menstrual cramps and breast tenderness and all of those types of symptoms. So, yep.
Dr. Justin Marchegiani: Very good. And then occult blood, we could see this potentially from blood in the stool, ulcerations, could be ulcerations in the stomach working its way down a lot of times I find It could be from hemorrhoids. It’s a common one too. The outer veins and the rectum area. They’re just, they’re dripping a little bit or the women out there on their menses too that could potentially drive that you’d be back there
Lisa Pomeroy: Exactly, yeah so ideally, I like to see under five that would be considered negative. 5-9 that’s where we often think oh, did you collect during your period, are you constipated, do you have hemorrhoids, no, that’s a typical range, anal fissures, maybe a constipated there’s a little tear or something. Above a 10 that’s our red flag because above a 10 we have to consider that you know this could be IBD, colorectal cancer, polyps and we just don’t want to miss any kind of pathology here. So, this is where we look to see is there something that makes sense or a diagnosis that makes sense say I see an occult blood of 35 well the person has ulcerative colitis. Okay now, we know why there may be blood it makes sense. But if it’s a 35 and there’s no known reason for this to be then we may need to repeat it, you know some of the acute pathogens again. If we go back to page one that E. coli, you know, uh, the 0157. That one can cause bloody stool. So, say that they got this nasty E. coli from a hamburger. Yep. And the, the EHEC, the enterohemorrhagic E. coli. Yeah. So, they could cause bloody stool so maybe, if there was a little bit of blood it was from an E. coli or something just passing through. So, if it’s above a 10 we often start by just repeating the occult blood to see was it some fluky thing where it was an acute pathogen or something but if you get two positive occult bloods it’s often referring out to see, you maybe need a colonoscopy because again we just don’t want to miss, we’ve caught early-stage colon cancer by catching some of these, you know, occult blood levels that are creeping up.
Dr. Justin Marchegiani: uhum, absolutely. And then we have IgA which is gonna be an immune marker that’s you, your kind of your mucosal membrane that kind of hits all the mucuses, so mouth, intestinal tract, vaginal canal, urinary canal, so if we see something high, that could be some kind of an immune stress. Your immune system is fighting and going after, if it’s low it could be just chronic stress that’s depleted that immune system that made you more vulnerable. Any thoughts on that?
Lisa Pomeroy: Yeah, exactly. I mean for me, low is a much bigger problem than high. High means the immune system’s working.
Dr. Justin Marchegiani: Working, yeah. It’s good.
Lisa Pomeroy: yeah. It’s attacking some microbe or some food but I mean that’s what it’s supposed to do, if something’s threatening it, it should go up, it should try to resolve it. Low means that it’s just it’s burnt out from wear and tear that constant assault and it just can’t mount a response and when it’s low you’re going to be more vulnerable to the E. coli and the Yersinias and the H. Pylori and the parasites because this is our first line defense, you know, we got to have this nice and robust.
Dr. Justin Marchegiani: Absolutely and then gluten antibodies, how often do you see this positive and I find it’s gonna drop if someone’s on a healthy diet they could still be gluten sensitive but it will go down so it may not be the best indication of hey, you're gluten sensitive, um, and you may get a false security because you kept your guten out and then you’re thinking, you’re okay and you can add it back in but it’s gonna be kind of exposure based, right?
Lisa Pomeroy: Exactly, yep. In order for the body to produce antibodies to something, it has to have that current exposure. Now, gluten antibodies can last three to six months in the system from a single exposure, so if they’ve had gluten in the last three to six months it could still be elevated from that but if someone if say they come in and they say I’ve been gluten free for five years, I shouldn’t be seeing elevated antibodies. If I am, there is a problem, it’s sneaking in somehow and we do often see this. I saw, I think two people earlier today who were diagnosed celiacs and it was high. That’s not good. That means that they’re still having that exposure so we’ve got to figure out where it’s coming from that is not a good thing and they’re telling you, really have to
Dr. Justin Marchegiani: Yeah, and what do you do when people are like, no I really haven’t been getting exposed. I tend to say well, is there cross contamination, is it potentially going high because maybe there’s an egg allergy or they’re eating some rice that’s technically gluten-free but could still react or is it still dairy thing what other foods could trigger that?
Lisa Pomeroy: Yeah, so first I look for actual gluten cross contamination because most cases it’s actually gluten, they didn’t realize that the oats, oats will be contaminated with gluten unless they’re certified gluten-free so it could be they’re eating their regular old quaker oats, you know, they’re gonna have gluten, so we gonna look for those or they’re sprouted bread. Yeah, it’s Ezekiel bread. It may have less gluten but still has gluten so we gotta look for that or oh my boyfriend eats gluten and I kiss him right after I, you know, after he eats the hamburger. That’s gonna be a step.
Dr. Justin Marchegiani: That’s possible.
Lisa Pomeroy: Or they kissed their dog, they feed their dog, regular gluten kibble and they kiss their dog. So, I looked at all of those, um, and they found that you know, eating out in restaurants. They did this great study a couple years back and they said about a third of all restaurant meals that you’re being told are gluten-free tested positive when they’re actually tested and that went up to 50% for gluten-free pizza and gluten-free pasta. So basically, if you go out to a restaurant, you order the gluten-free pizza or pasta, it’s a 50 50 shot whether you’re actually getting gluten or not.
Dr. Justin Marchegiani: Yeah. It tends to be, usually if you’re going out, if you’re getting like a steak or some steamed vegetables, usually you’re okay tends to be more in the sauces, the thickeners or even a spice and so worst case you just, you season it yourself with your own sea salt at the table or something just to make sure it’s its clean.
Lisa Pomeroy: And some things too, I mean I actually you know because I am gluten sensitive, you know, gluten triggers Hashimoto’s for me. So, I went gluten-free like 14 years ago and my antibodies dropped and never come back because I’ve stayed gluten free.
Dr. Justin Marchegiani: That’s great.
Lisa Pomeroy: But I do test. I have this little testing device and you could put a pea sized portion of the food in the device, it takes about three minutes and it’ll tell you if it had gluten or not. So, I will test if I buy some new food, especially if it says manufactured in the same warehouse with wheat, dairy and all that kind of stuff or if I don’t know say if I want to eat, I can put the food in the device and know if its gluten-free or not. So
Dr. Justin Marchegiani: Wow, so what’s this device called?
Lisa Pomeroy: It’s called Nima. It’s N-I-M-A. So, it’s a Nima, Nima Partners Company, you can buy it through. It’s cool little device, you have to buy these capsules that are one-time use but you put the food in the device, so anytime I buy anything new any packaged food, even supplements, I run it through my Nima. Because, I was being glutened by a cinnamon powder like I run one of these tests on myself and my anti-gliadin was a little high and I thought was a test wrong that this is impossible I’ve, I’ve been gluten free for over a decade this got to be wrong so I bought a Nima then this a few years back and tested everything I was eating and an organic cinnamon powder the company grinds fresh in their facility tested positive and I was eating this almost every day. I stopped eating it, seven months later retested, antibodies gone.
Dr. Justin Marchegiani: Wow, okay. We’ll put a link up on screen put it on the show notes that’s uh, that’s crazy, very cool.
Lisa Pomeroy: If I’ve ruled out that, that’s the first thing I look for because the majority of people, it is just gluten contamination. Now if we’ve ruled that out then I looked at okay there’s about six foods that are cross-reacted with gluten, there’s dairy, there’s yeast, there’s corn, there’s millet. So, then we start to look at
Dr. Justin Marchegiani: other things
Lisa Pomeroy: Yep. Other things that you know if you’re continuing to eat dairy then maybe there’s an issue there. Yeah, it’s, they recently changed the website, I think it’s Nimapartners.com
Dr. Justin Marchegiani: Okay cool. I’ll put it below in the show notes. Anyone’s listening back and you’ll get that. That’s great.
Lisa Pomeroy: So sometimes we have to remove cross-reactive foods so there can be other factors but you know, the problem is once you’ve lost oral tolerance to gluten, you can’t get it back. It’s the only food we know of that your body creates memory B cells to so, it is something like for me being gluten-free for like 14 years I shouldn’t have antibodies but if I start eating gluten again, I will have antibodies because I’ve lost oral tolerance.
Dr. Justin Marchegiani: That’s why I like the genetic test because you don’t have to necessarily challenge it or know you, if you have the HLA DQ2 or eight or you know one alpha, one beta, one or three then it’s a good chance that you have that those gluten sensitivities and you should probably stay away from it.
Lisa Pomeroy: Um, yeah.
Dr. Justin Marchegiani: Any feedback on the genetic testing for the gluten.
Lisa Pomeroy: Yeah, I think it’s helpful, I like all these tests, I mean they always give you a little different piece of information so I think it’s helpful, you know a lot of times correlating the genetics with what we’re seeing here. So, I mean the genetics don’t tell you, you are having a problem versus this tells you are having a current problem. So, I like both and sometimes people need the information from both because just seeing the genetics, you know, they go, well I could have a problem but is that enough you know, a motivational factor to keep me from eating gluten versus I see this and it’s high then I know, okay, my body is really not happy right now because of the gluten I’m eating. I definitely need to go gluten-free. So, it depends what motivates someone and again if they haven’t eating gluten for a while, I don’t want them challenging it, you know, they could certainly again run this as is like myself eating the cinnamon, I though, I was gluten free but I was being glutened so it showed up. So, I tell people run the test as is look at your genetics and I’d rather you do that than reintroducing gluten and now starting that inflammatory cascade that’s going to last for three to six months.
Dr. Justin Marchegiani: Very cool. Well let’s just wrap this up, your last couple of markers and by the way, I know we chatted about, uh, probably a little bit ambitious wanting to go into the, uh, the ion panel but I’d love to have you back soon, Lisa and really dive into the ion panel. Would you be open to that?
Lisa Pomeroy: I would, I love talking lab test interpretation.
Dr. Justin Marchegiani: Very cool, so out of the gate here, calprotectin, really good tests for inflammation produced by the white blood cells in the intestinal tract, it’s a protein and of course, Zonulin is that protein, that’s a sign that those tight junctions are being unzipped in the intestinal tract and potential gut permeability. Comments on that?
Lisa Pomeroy: Yeah. So, calprotectin is a kind of a general marker for intestinal inflammation. Now with IBD, we can see this exceptionally high. Usually, yeah, the two things that are going to cause your highest levels are acute pathogens so again something like that nasty food poisoning E. coli or something like your IBD type thing. You could see upper hundreds or even thousands with that.
Dr. Justin Marchegiani: Yeah
Lisa Pomeroy: Ideally, I wanna see under 50. So, a lot of people will see things like an 87 or a 120 where I go that’s higher than I’d like, so again, we start looking at, okay, what’s causing this colonic inflammation, again, are you lacking butyrate producers, do you have too many of these proinflammatory bugs, do you have a parasite like Blasto hanging out in your colon. So, we’re looking at all those other factors that could be causing inflammation. Or again, some of the food additives, you know, maybe you like to go your grocery store and get rotisserie chicken. A lot of rotisserie chickens have Carrageenan in them. Carrageenan is a known proinflammatory food additive. So, there’s little things we can sometimes do to bring down our gut inflammation but yeah, so that one’s gonna tell you about if your gut is inflamed or not, Zonulin tells you if your gut is leaky. Now Zonulin will, you know, go up, you know, it’s triggered by things like gluten and gram-negative bacteria. They have an endotoxin, LPS in them. So, gluten and LPS are the top two triggers for Zonulin, so again I’m looking for is antigliadin high, do you have a lot of these bacteria that are overgrowing or again do you eat GMO foods like glyphosate is another trigger for Zonulin. So, if this is high, we need to look for, what’s triggering it and then we’re probably gonna need to do some gut repair, you know, maybe we want an L-glutamine based powder, you know, because we want to make sure that the gut damage is being healed up the tight junctions are restored, the integrity of the gut barrier is restored.
Dr. Justin Marchegiani: Very cool. And then Lisa, you’ve given us so much information here. This is excellent. I’m going to recommend this to my patients here to get a kind of a little bit more of a deeper dive, if they want more intel. This is excellent. Um, if people wanna find out more about you, where’s the best place to go?
Lisa Pomeroy: Yeah. So, I have a couple different websites, I work with practitioners and right now I’m, you know my practice is closed to taking in new clients but, you know, may open up in the future, so my more client website is my last name Pomeroy, so pomeroynaturalhealth.com. Now, if there are practitioners who want more, you know, help on lab interpretation for their patients or if they’re interested in the different training courses I created, that website for practitioners is pomeroyinstitute.com
Dr. Justin Marchegiani: pomeroynaturalhealth.com for patients. pomeroyinstitute.com for practitioners. We’ll put the links below here, so people can get to that faster. Anything else you want to leave listeners today with, Lisa?
Lisa Pomeroy: Um, I guess, just you know, they say all health begins in the gut and I’m a believer of that because I had so many issues, I mean, you almost name a pathogen on this report I’ve had it. Everything from roundworms to just about every Protozoa to H. pylori. You know, I’ve had it all and I know how much, you know, it just wreaked havoc on my gut for decades so starting very young. You know, my parents would always think she’s coming down with a stomach flu because she just puked out of the blue. You know, it was just the H. pylori and everything else, my low enzymes. So, I had just terrible terrible gut and so I mean for me was the functional lab testing that found these issues. I mean, that found the H. pylori, the parasites, the low enzymes, everything else and I just think you know for me it’s just so important on why I get so passionate about this. For me, it was giving me the answers that I needed to restore my health. So
Dr. Justin Marchegiani: Excellent. Well, you have a great story at least, you did an excellent job for sending me information and I think uh, people that are watching are getting a lot of information out of it. So really appreciate it, look forward to have you back on the show real soon.
https://pomeroynaturalhealth.com/
